Types of Anaesthesia: a guide for Australian patients
In Australia, anaesthesia is delivered by specialist anaesthetists with more than 12 years of medical and specialist training. There are four main categories — general, regional, local, and sedation — and the right choice depends on your procedure, your health, and your preferences.
The four ways anaesthesia is given in Australia — general, regional, local, and sedation — illustrated as four moments of care for the same patient.
4
Main categories of anaesthesia in routine use
~5M
Procedures involving anaesthesia in Australia each year
12+
Years of training required to become a FANZCA
100%
Delivered by a specialist anaesthetist or supervised trainee
Use this table to compare the main categories on the dimensions patients ask about most. Scroll horizontally on mobile.
General
Regional
Local
Sedation
Consciousness
Unconscious
Awake (sedation optional)
Fully awake
Drowsy to deeply asleep
What you feel
Nothing
Numbness in the region; no pain
Numbness at the site; no pain
Relaxed; usually no pain
Memory of procedure
None
Awareness of theatre, no pain
Awake, may watch
Usually little or none
Breathing
Managed by anaesthetist
Your own
Your own
Your own (closely monitored)
Typical use
Major surgery; long procedures
Limbs, lower body, childbirth
Skin, dental, small procedures
Endoscopy, cataract, minor work
Recovery focus
Drowsiness, sore throat possible
Numbness wears off over hours
Minutes to a few hours
Clears within 1–2 hours
Who delivers it
Specialist anaesthetist
Specialist anaesthetist
Surgeon, GP, dentist or anaesthetist
Anaesthetist or accredited sedationist
This table summarises typical practice in Australia. Your anaesthetist will tailor the plan to your individual situation.
Interactive · Procedure explorer
Which anaesthesia is typical for your procedure?
Pick a common procedure to see the anaesthesia type(s) most often used in Australian practice, what to expect, and how recovery typically goes. This is a general guide — your anaesthetist makes the final plan.
Don't see your procedure? The four broad categories below cover almost every scenario.
Cataract surgery
Typical Australian practice
Loading...
You will be
—
Memory of the procedure
—
Typical recovery
—
Day stay or admission
—
Important: This explorer reflects the most common Australian approach. Your anaesthetist may recommend a different plan based on your health, the surgeon's preference, the facility, and your wishes. Always discuss the specifics of your case at your pre-anaesthetic consultation.
Detailed guide
Each type, in depth
The same four categories, but with the detail patients actually want: how each works, what you'll feel, common uses, and what recovery is like.
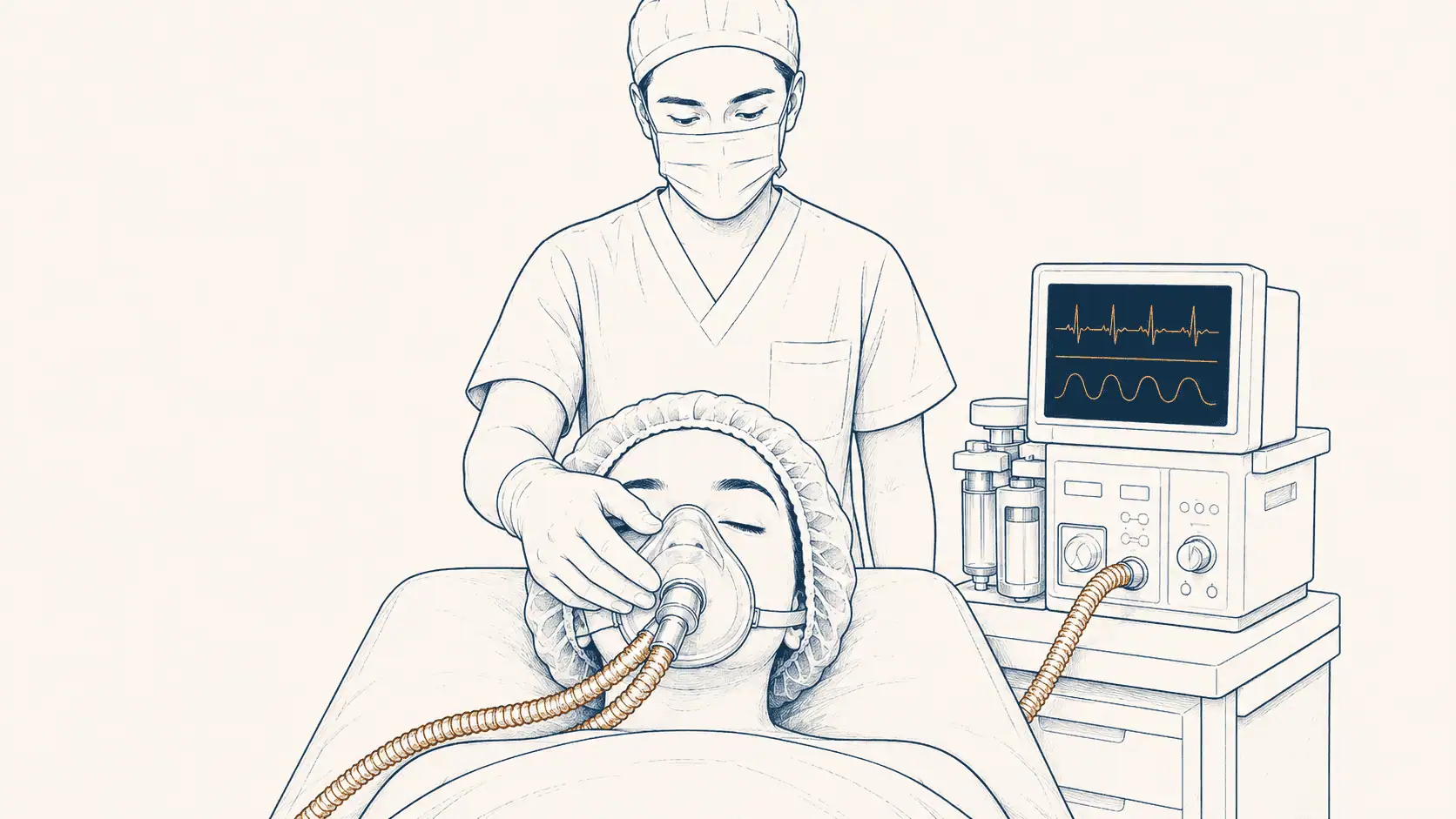
General anaesthesia
A medically induced, carefully controlled state of unconsciousness. You are completely unaware of the procedure and feel nothing.
How it works
Your anaesthetist gives a combination of medications — typically through an intravenous (IV) line in your hand or arm, sometimes followed by anaesthetic gases inhaled through a mask or breathing tube. Within seconds, you lose consciousness. The anaesthetist continuously monitors your heart rate, blood pressure, breathing, oxygen levels, and depth of anaesthesia, adjusting medication throughout the operation.
What you'll feel
You will remember being in the anaesthetic room, possibly counting backwards or feeling a brief stinging sensation as the IV medication goes in. The next thing you experience is waking in the recovery room. Most people describe it as time skipping forward — there is no sense of the operation having taken place.
Commonly used for
Major abdominal, chest, and intracranial surgery
Long operations or those requiring deep muscle relaxation
Procedures in patients who can't tolerate being awake (children, anxiety)
Most laparoscopic ("keyhole") surgery
Recovery
You will spend 30 to 90 minutes in the recovery room as the anaesthetic wears off and pain relief is established. Most people are alert and oriented within an hour. Feeling completely back to normal — full concentration, energy, and reflexes — typically takes 24 hours. Driving, signing legal documents, and operating machinery should be avoided for 24 hours after a general anaesthetic.
Things to know
A sore throat (from the breathing tube), nausea, drowsiness, and shivering are common but short-lived. Awareness during general anaesthesia is uncommon and your anaesthetist continuously adjusts medication to prevent it. Serious complications in a healthy patient having routine surgery are uncommon.
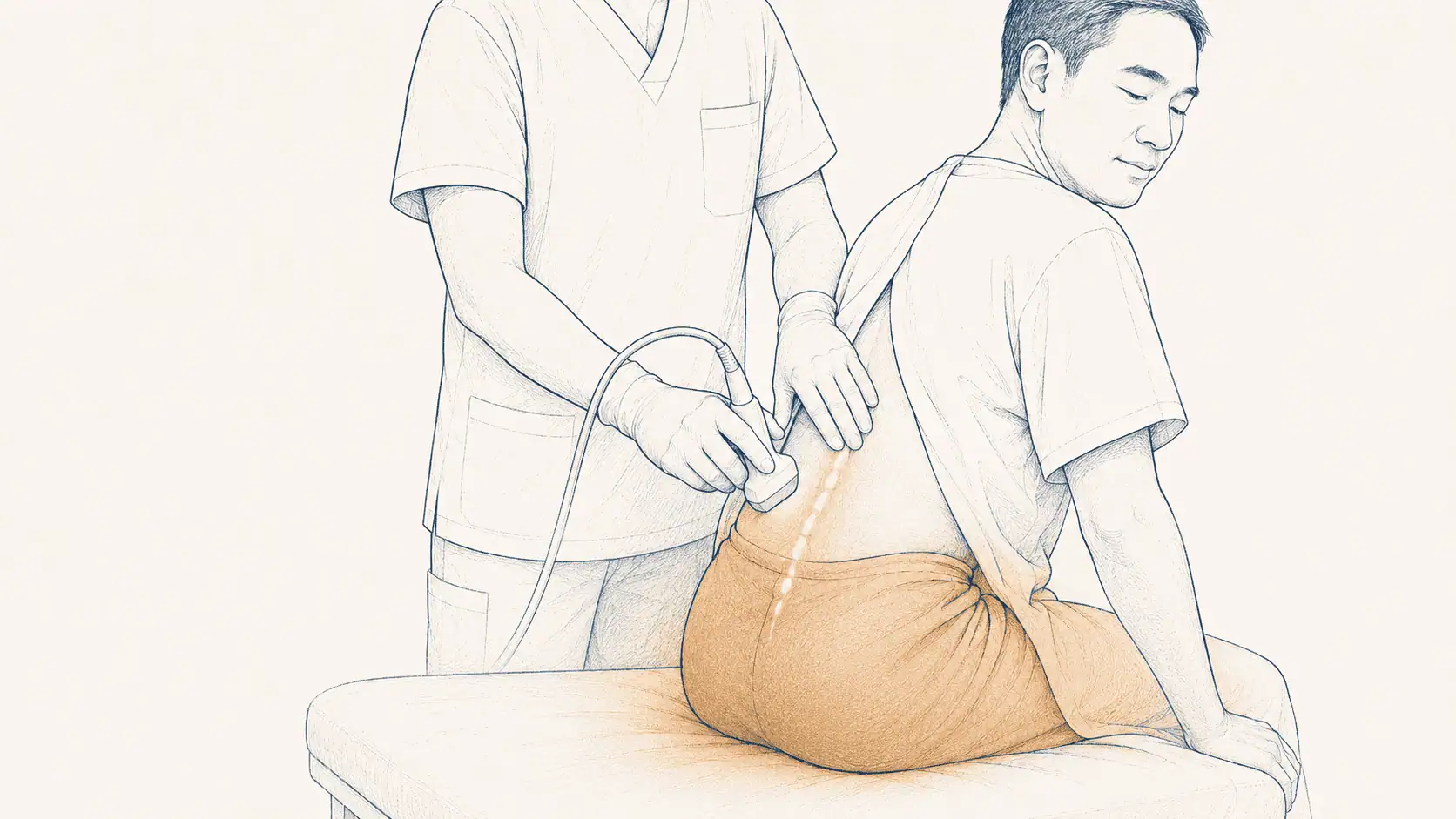
Regional anaesthesia
Local anaesthetic is injected around a major nerve or group of nerves, completely blocking pain from a region of the body. You stay awake unless you also have sedation.
How it works
Your anaesthetist uses ultrasound (or sometimes a nerve stimulator) to guide a small needle close to the nerves supplying the operative area. A local anaesthetic such as ropivacaine or bupivacaine is injected; within minutes the region becomes numb and heavy. The block can last anywhere from one hour to a full day depending on the drug used, and can be extended further by leaving a fine catheter in place.
Main subtypes
Spinal anaesthesia — a single injection of local anaesthetic into the fluid around the spinal cord. Numbs everything from the waist down within minutes. Standard for elective caesarean section and many lower-limb operations.
Epidural anaesthesia — a small catheter is placed just outside the spinal sac, allowing top-up doses. Used widely for pain relief in labour and after major abdominal or chest surgery.
Peripheral nerve blocks — targeted injections near specific nerves (brachial plexus for shoulder/arm, femoral or popliteal for the leg, paravertebral for the chest, and so on). Often used with general anaesthesia to provide post-operative pain relief.
What you'll feel
You'll feel a brief sting as the local anaesthetic is injected into the skin, and possibly some pressure or pins-and-needles as the block sets in. The operative area then becomes numb and you cannot move it or feel pain. You can usually still feel touch and pressure, but not sharpness.
Recovery
You avoid most of the side effects of general anaesthesia (drowsiness, sore throat, nausea), and pain relief continues for hours after the operation. Numbness usually wears off in 4 to 24 hours; for spinals, you may need to stay until you can move your legs and walk — passing urine before discharge is sometimes required. There is some evidence that regional anaesthesia is associated with less post-operative nausea and reduced opioid use.
Things to know
Headache after a spinal is uncommon but possible. Permanent nerve injury from regional blocks is very rare. If you are anxious about being awake, sedation can be added so you doze through the procedure — many patients prefer this.
Local anaesthesia
A small amount of local anaesthetic is injected at or near the surgical site, numbing only that area. You stay fully awake and aware.
How it works
An agent such as lignocaine (sometimes mixed with adrenaline to make the effect last longer) is injected into the skin and underlying tissue at the surgical site. Within a minute or two, the area is numb. The dose used is small, so the effect stays local — your wider body is not affected.
What you'll feel
A brief stinging or burning as the local goes in. After that, you'll feel pressure and movement at the site but no sharpness or pain. You can talk, watch, and respond throughout. There is no drowsiness afterwards.
Cataract surgery (as topical drops, often combined with light sedation)
Recovery
Almost none. You walk out, drive home, and resume normal activity. The numbness typically wears off in one to three hours, depending on the agent. There is no anaesthetic "hangover".
Things to know
Local anaesthesia alone is best suited to small, short procedures. For anything longer or more uncomfortable, your doctor may suggest combining local with sedation so you stay relaxed. Local anaesthetic is administered by surgeons, GPs, dentists, and emergency physicians as well as by anaesthetists.
Sedation & Monitored Anaesthesia Care (MAC)
Medications make you relaxed, drowsy, and often forgetful of the procedure. You typically breathe on your own. Sometimes called "twilight" anaesthesia.
How it works
Your anaesthetist gives a carefully titrated combination of medications (such as midazolam, fentanyl, and propofol) through an IV. A small amount of supplemental oxygen is delivered via nasal prongs or a mask. Throughout, your anaesthetist monitors your breathing, heart rate, blood pressure, and oxygen levels — the "monitored" part of Monitored Anaesthesia Care.
Levels of sedation
Minimal — relaxed but fully awake. You can answer questions normally.
Moderate ("conscious sedation") — drowsy and possibly asleep. You respond to voice or light touch.
Deep — asleep, responding only to firm stimulation. Breathing may need support.
General anaesthesia — if sedation becomes deep enough that you cannot maintain your own airway, it crosses over into general anaesthesia. Your anaesthetist is trained to manage this safely.
Commonly used for
Colonoscopy and gastroscopy
Cataract surgery (combined with local)
Minor cosmetic and plastic procedures
Interventional radiology and cardiology
Some dental work in anxious patients
Recovery
Most people are awake and able to chat within 5 to 15 minutes. You'll spend 30 to 60 minutes in recovery before going home, accompanied by a responsible adult. No driving, drinking alcohol, or signing legal documents for 24 hours.
Things to know
Most patients remember little or nothing — the sedative medications cause short-term amnesia. Deep sedation has many of the same considerations as general anaesthesia, which is why having a specialist anaesthetist managing it adds an important layer of safety.
In practice
Anaesthesia is often a combination
The four categories are rarely used in isolation. Combining techniques is standard practice and often gives the best results — better pain control, faster recovery, fewer side effects.
Most common
General + nerve block
For knee replacement, shoulder surgery, or breast surgery, a nerve block is often placed before or during general anaesthesia. You wake up with the operative area already numb — and stay comfortable for many hours afterwards with less need for opioids.
Standard for many day cases
Local + sedation
The local anaesthetic does the heavy lifting (no pain at the site), while light sedation handles anxiety and discomfort. Standard for cataract surgery, many plastic procedures, and some endoscopies.
Major surgery
General + epidural
For major abdominal or chest surgery, an epidural is often placed before induction and left in place for several days post-op. This dramatically improves pain relief, helps you breathe more easily, and can speed up recovery.
Caesarean section
Spinal + light sedation (rarely)
Elective caesarean is almost always done under regional anaesthesia — usually a spinal block, sometimes a combined spinal-epidural. You stay awake and your partner can be present. Sedation is typically avoided so you can be alert for the birth. General anaesthesia is reserved for emergencies or when regional anaesthesia isn't possible.
Standards
Who delivers anaesthesia in Australia
In Australia, specialist anaesthesia is delivered by a Fellow of the Australian and New Zealand College of Anaesthetists (FANZCA) or by a supervised anaesthesia trainee. To become a FANZCA, a doctor must complete:
A medical degree (typically 4–6 years)
At least 2 years working as a junior doctor (intern and resident)
At least 5 years of accredited specialist anaesthesia training — comprising 2 years of introductory and basic training, 2 years of advanced training, and 1 year of provisional fellowship — including the ANZCA primary and final examinations
In total, a FANZCA has had more than 12 years of medical training before practising independently. Once qualified, anaesthetists are required to keep their skills current through ANZCA's CPD program. ANZCA also sets the professional standards for monitoring, equipment, and conduct of anaesthesia in operating theatres across Australia.
Modern anaesthetic practice in Australia is among the safest in the world. The vast majority of patients have a smooth procedure and an uncomplicated recovery. Some perspective on the most common risks:
Common
Sore throat, nausea, drowsiness, shivering
Short-lived. Anti-nausea medication is routine.
Uncommon
Dental damage, minor nerve irritation, post-dural-puncture headache
Usually resolves with conservative management.
Rare
Awareness during general anaesthesia
Uncommon. Modern depth-of-anaesthesia monitoring reduces this further.
Very rare
Serious allergic reaction, permanent nerve damage, anaesthetic-related death
In healthy patients having routine surgery, very uncommon.
Your anaesthetist will assess your individual risk before any procedure based on your age, medical conditions, medications, and the surgery itself, and will discuss any concerns with you at your pre-anaesthetic consultation.
Common questions
Patient FAQ
The questions patients ask us most often before surgery. Tap any question to reveal the answer.
Will I feel pain during surgery under anaesthesia?
No. Whichever type of anaesthesia is used, the goal is for you to be free of pain during the procedure. Under general anaesthesia you are unconscious and have no awareness. Under regional or local anaesthesia, the specific area is numbed so you feel no pain even though you may stay awake. Sedation is often added so you feel relaxed and remember little.
Will I wake up during surgery under general anaesthesia?
Awareness during general anaesthesia is uncommon. When patients are asked about it directly after surgery, studies report it in around 1–2 per 1,000 general anaesthetics; when measured by spontaneous reports, the rate is much lower — UK national audit data put it at around 1 in 20,000. Modern depth-of-anaesthesia monitoring and continuous adjustment of medication further reduce the risk.
How long does anaesthesia take to wear off?
It depends on the type. Most general anaesthetics wear off within 15 to 30 minutes of the operation ending, although feeling fully back to normal can take 24 hours. Sedation typically clears in one to two hours. Local and regional anaesthesia can last from one to 24 hours depending on the agent and the technique used.
What's the difference between sedation and general anaesthesia?
Sedation makes you relaxed and drowsy but you can usually still respond to the anaesthetist. General anaesthesia is a controlled state of unconsciousness — you are completely unaware, and the anaesthetist manages your breathing and circulation. Deep sedation sits between the two and can resemble general anaesthesia.
Can I choose which type of anaesthesia I have?
For many procedures there is more than one safe option, and your preferences matter. Your anaesthetist will discuss the choices, the pros and cons of each, and recommend what suits your health and the procedure best. For some operations only one type is suitable, in which case your anaesthetist will explain why.
Is anaesthesia safe?
Modern anaesthesia in Australia is very safe. The risk of a serious adverse event in a healthy patient having routine surgery is very low. Risk increases with age, complex medical conditions, and the complexity of the surgery itself. Your anaesthetist will assess your individual risk before any procedure.
Why do I need to see an anaesthetist before surgery?
The pre-anaesthetic consultation lets your anaesthetist review your medical history, medications, allergies and airway, choose the safest anaesthetic plan, and answer your questions. For straightforward day surgery this is sometimes done on the day; for complex surgery it usually happens days or weeks beforehand.
Will I remember the procedure if I have sedation?
Most people remember very little or nothing of a procedure done under sedation. Many of the medications used cause short-term amnesia. The depth of sedation also affects memory — deeper sedation means less recall.
What are the most common side effects after anaesthesia?
Common short-lived side effects include drowsiness, a sore throat (after a breathing tube), nausea, shivering, and a mild headache. These usually settle within a few hours. Anaesthetists can offer medication to prevent or treat nausea if you have had problems with it before.
Will an anaesthetist be with me the whole time?
Yes. In Australia, a specialist anaesthetist (or appropriately supervised anaesthesia trainee) stays with you continuously from the start of anaesthesia until you are handed over to recovery staff, in line with ANZCA professional standards.
BH
Reviewed by
Dr Brad Hindson, FANZCA
Dr Hindson is a specialist anaesthetist and Fellow of the Australian and New Zealand College of Anaesthetists, and founder of Fast Tracking Anaesthetic Billing Services. He has reviewed this article for clinical accuracy in line with current Australian practice.
Last reviewed: 15 May 2026·Next review due: November 2026·About the author
Medical disclaimer. This article is for general information only and is not a substitute for individual medical advice. If you have specific concerns about anaesthesia for your procedure, please discuss them with your anaesthetist, surgeon, or GP.
Fast Tracking handles billing for hundreds of anaesthetists across Australia. If you have a question about an invoice, a Medicare rebate, or your fund cover, our team can help.